Almost everyone has felt it at some point: that burning sensation rising behind the breastbone after a large or late meal, often called heartburn. When it happens occasionally, it is simple acid reflux. When it becomes frequent and troublesome, it has a name of its own, gastroesophageal reflux disease, or GERD. Behind the discomfort is a small but important valve at the top of the stomach that is letting acid escape upward into the esophagus, where it does not belong. The encouraging news is that reflux is one of the most responsive conditions to changes in eating and lifestyle, and effective medicines exist for the times when those changes are not enough. In this article I explain what acid reflux and GERD are, which organs they affect, how the condition develops, its strong link with diet, and how it can be calmed by natural and medical means.
Table of Contents
- What is acid reflux and GERD?
- What are the symptoms?
- Which organs does it affect?
- Progression: from occasional reflux to GERD
- How it presents and is diagnosed
- Causes and risk factors
- Its relationship with nutrition
- The place of fats
- Natural foods that help calm reflux
- Calming reflux by natural means
- Where to find natural support
- When medical treatment is needed
- Small but effective daily changes
- A final word
What is acid reflux and GERD?
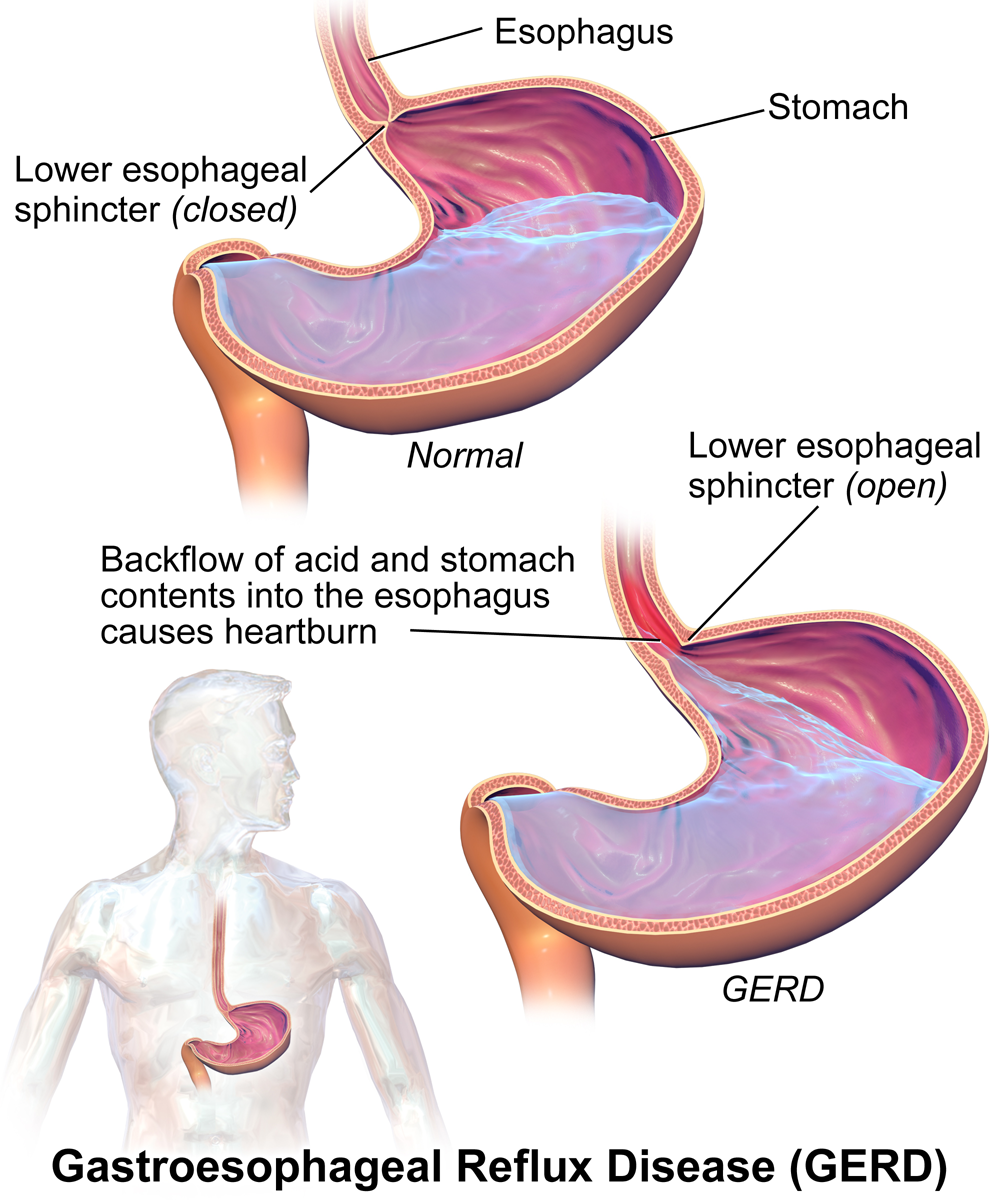
To understand reflux, it helps to picture the gateway between the esophagus and the stomach. At this junction sits a ring of muscle called the lower esophageal sphincter. Normally it works like a one-way valve: it opens to let food pass down into the stomach, then closes tightly to keep the stomach’s acidic contents from travelling back up. Gastroesophageal reflux, or GER, is simply what happens when that valve briefly relaxes and a little stomach content escapes upward.
Occasional reflux is completely normal and almost everyone experiences it now and then, especially after a big meal. It becomes gastroesophageal reflux disease, or GERD, when the reflux happens frequently, causes bothersome symptoms, or begins to irritate and damage the lining of the esophagus. In other words, GERD is reflux that has crossed the line from an occasional nuisance into a persistent medical condition.
The reason it matters is that the esophagus, unlike the stomach, is not built to withstand acid. The stomach has a tough, protective lining; the esophagus does not. When acid washes up repeatedly, it irritates this delicate tissue, producing the familiar burning and, over time, potentially more serious changes. Understanding GERD as a problem of a leaky valve, rather than simply too much acid, is the key to managing it well.
What are the symptoms?
The most recognisable symptom of reflux is heartburn, a painful, burning feeling in the middle of the chest, behind the breastbone, that can rise toward the throat. It often appears after meals, when lying down, or when bending over. The second classic symptom is regurgitation, where stomach contents come back up into the throat or mouth, sometimes bringing a sour or bitter taste of acid or food.
Not everyone with GERD has these obvious symptoms, however, and the condition can show up in less expected ways. Some people experience chest pain, nausea, or trouble and pain when swallowing. Others have what are sometimes called the silent or atypical symptoms: a chronic cough, hoarseness, a sensation of a lump in the throat, or repeated throat clearing, caused by acid irritating the throat and airways.
Certain symptoms are warning signs that call for prompt medical attention rather than self-treatment. These include difficulty or pain swallowing, persistent vomiting, unexplained weight loss, loss of appetite, or any sign of bleeding such as vomit that looks like coffee grounds or black, tarry stools. Chest pain in particular should never be assumed to be heartburn without medical assessment, since it can mimic heart problems. When in doubt, it is always safest to get checked.
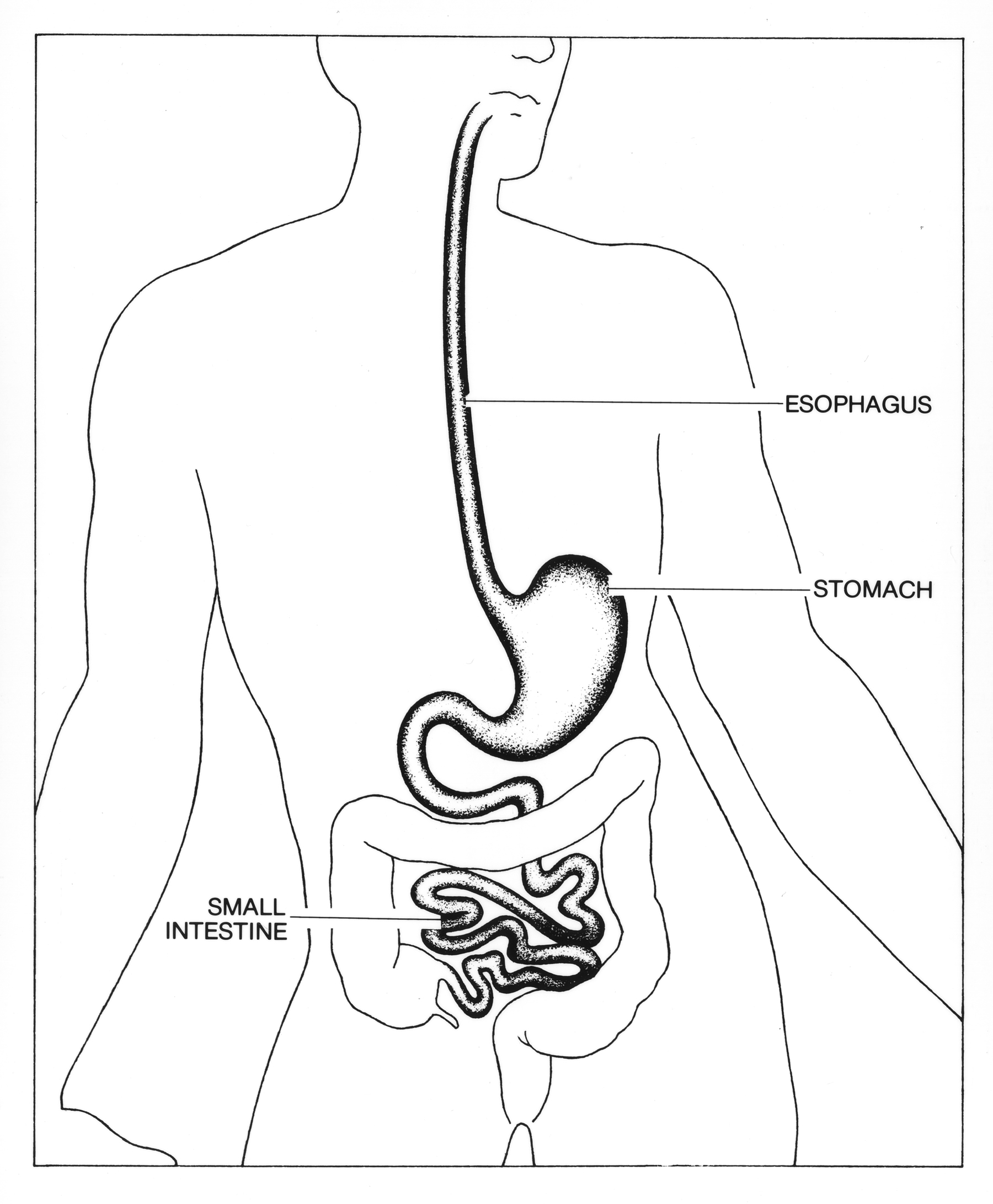
Which organs does it affect?
The esophagus is the organ at the centre of GERD, and it bears the brunt of the damage. Repeated exposure to acid can inflame its lining, a condition called esophagitis, leading to soreness, painful swallowing, and sometimes small erosions or ulcers. Over a long time, the irritation can cause narrowing, known as a stricture, that makes swallowing difficult.
But the reach of reflux extends beyond the esophagus. Acid that travels high enough can affect the throat and voice box, causing hoarseness and chronic throat irritation, and it can reach the airways, triggering or worsening a chronic cough and even contributing to asthma-like symptoms in some people. This is why reflux is sometimes first suspected by an ear, nose, and throat specialist or a lung doctor rather than a stomach specialist.
The mouth is not spared either; long-standing acid exposure can erode tooth enamel. Perhaps most important is the small minority in whom years of untreated GERD lead to changes in the esophageal lining called Barrett’s esophagus, which slightly raises the long-term risk of a particular esophageal cancer. This is uncommon and develops slowly, but it is the main reason persistent reflux deserves proper attention rather than being endlessly self-medicated.
Progression: from occasional reflux to GERD
Reflux exists on a spectrum. At the mild end is the occasional heartburn that most people get after an indulgent meal, which resolves on its own and causes no harm. There is nothing to treat here beyond common sense, and it is not a disease.
The picture shifts when reflux becomes frequent, typically defined as happening more than a couple of times a week, or when it starts to interfere with daily life and sleep. At this stage it qualifies as GERD. The lining of the esophagus may begin to show inflammation, and symptoms become a recurring problem rather than an occasional one.
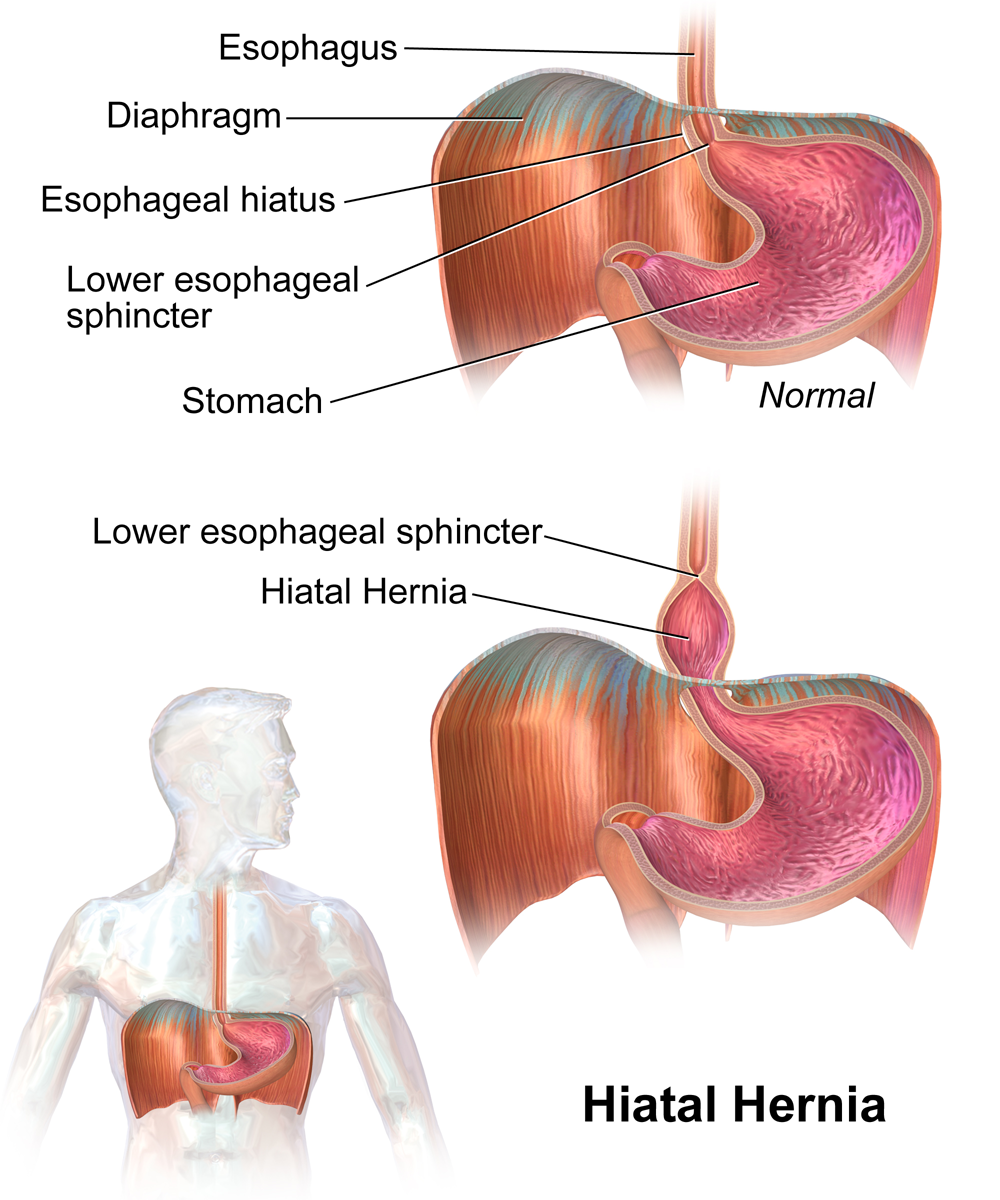
If GERD goes unmanaged for a long time, complications can slowly develop, including esophagitis, strictures, and, in a small number of people, Barrett’s esophagus. A hiatal hernia, where the upper part of the stomach pushes up through the diaphragm, can make reflux worse and is often found alongside more troublesome GERD. The key message is that this progression is usually slow and largely preventable, which is exactly why catching and managing frequent reflux early is so worthwhile.
How it presents and is diagnosed
For most people, GERD presents simply as recurring heartburn and regurgitation, and doctors can often make the diagnosis from the typical symptoms alone, especially when those symptoms improve with a trial of acid-reducing treatment. There is no need for invasive tests in straightforward cases.
Further investigation is reserved for certain situations: when symptoms are severe, do not respond to treatment, or are accompanied by warning signs such as difficulty swallowing or weight loss. In these cases a doctor may recommend an endoscopy, in which a thin, flexible tube with a camera is passed down to look directly at the esophagus and stomach, checking for inflammation, ulcers, or Barrett’s changes. Other specialised tests can measure how much acid actually refluxes and how the esophagus moves.
This stepwise approach, treating the common case simply and investigating only when there is reason to, is sensible and reassuring. Most people never need anything more than a conversation with their doctor and a trial of lifestyle changes and medicine. The tests exist for the minority who need a closer look, ensuring that the small number of more serious cases are not missed.
Causes and risk factors
At its core, GERD develops when the lower esophageal sphincter becomes weak or relaxes when it should stay closed. Several factors push in this direction. Being overweight or obese is a major one, because extra abdominal pressure tends to force stomach contents upward. Pregnancy does the same through both pressure and hormonal changes, and smoking weakens the valve as well.
A hiatal hernia, where part of the stomach slips up through the diaphragm, removes some of the natural anti-reflux support and is a common contributor. Diet and eating habits play a large role too, which is covered in detail below. Some medicines can relax the sphincter or irritate the esophagus, including certain blood pressure drugs, some asthma medicines, sedatives, certain antidepressants, and anti-inflammatory painkillers.
The encouraging side of this list is how many of the strongest contributors are modifiable. Weight, smoking, eating patterns, and meal timing are all within a person’s control, which is precisely why lifestyle change is such a powerful first treatment. Recognising one’s own triggers, whether a particular food, late-night eating, or extra weight around the middle, is often the first step toward lasting relief.
Its relationship with nutrition
Few conditions are as closely tied to what and how we eat as reflux. Both the contents of a meal and the way it is eaten influence whether acid escapes upward. Large meals stretch the stomach and make the valve more likely to leak, so portion size matters as much as food choice. Eating late and then lying down gives gravity no chance to keep acid in the stomach, which is why night-time reflux is so common.
Certain foods are well known to relax the valve or stimulate acid and so tend to provoke symptoms in many people. These commonly include very fatty and fried foods, chocolate, peppermint, coffee and other caffeinated drinks, alcohol, carbonated beverages, and acidic or spicy foods such as tomatoes, citrus, and chilli. Triggers are quite individual, though, and not everyone reacts to the same foods, so paying attention to one’s own pattern is valuable.

Moving away from heavily processed, very fatty, and sugary foods, while building meals around vegetables, whole grains, lean protein, and non-citrus fruit, tends to settle reflux for many people. Smaller, more frequent meals, eaten slowly and not too close to bedtime, often help as much as changing the foods themselves. In this sense, managing reflux is as much about eating habits as it is about a list of foods to avoid.
The place of fats
Fat deserves a careful, balanced word in any discussion of reflux. On one hand, very fatty and fried meals are among the classic triggers, because fat slows stomach emptying and can relax the lower esophageal sphincter, giving acid more time and opportunity to escape. So it is true that heavy, greasy meals often make reflux worse.
On the other hand, it would be a mistake to conclude that all fat should be banished. Fat is an essential nutrient that the body genuinely needs. It builds the membranes of every cell, is a raw material for hormones, and is required to absorb the fat-soluble vitamins A, D, E, and K. The goal is not to eliminate fat but to choose the right kind and to keep portions moderate, since it is large, fatty meals, rather than fat itself, that most reliably provoke symptoms.
Healthy fats from olive oil, nuts, avocado, and fish, eaten in sensible amounts, are part of a nourishing diet and are very different from the spoiled and repeatedly heated fats in fried and ultra-processed foods. There is also a familiar trap: many “fat-free” and “low-fat” products replace the missing fat with extra sugar or refined starch, which adds empty calories without genuine benefit. For reflux, the wise approach is to favour quality fats in modest portions, avoid large greasy meals, and steer clear of processed substitutes, rather than fearing fat in every form.
Natural foods that help calm reflux
While trigger foods vary from person to person, several foods tend to be gentle on a reflux-prone stomach and are worth leaning on. High-fibre foods such as whole grains, oats, vegetables, and non-citrus fruits support healthy digestion and may help reduce reflux. Vegetables in general are naturally low in fat and sugar and rarely provoke symptoms.
Lean proteins such as poultry, fish, and legumes are usually well tolerated, especially when grilled, baked, or steamed rather than fried. Non-citrus fruits like bananas and melons, and watery foods that dilute stomach acid, are often soothing. Ginger has a traditional reputation for settling the stomach and is gentle for many people, and plain water between meals can help wash acid back down.
The common thread among reflux-friendly foods is that they are whole, minimally processed, and not excessively fatty, acidic, or spicy. Equally important is how they are eaten: in smaller portions, slowly, and well before lying down. Building everyday meals around this kind of pattern gives the stomach the best chance to keep its contents where they belong, and lets the esophagus heal between any flares.
Calming reflux by natural means
For many people, especially with milder GERD, natural and lifestyle measures are a powerful first line of treatment and can control symptoms without any medication. Losing excess weight is one of the most effective steps, because reducing abdominal pressure directly eases the strain on the valve. Even a modest weight loss can make a noticeable difference for those carrying extra weight.
Several simple habits help a great deal. Eating smaller meals, avoiding food in the two to three hours before bed, and not lying down straight after eating all work with gravity rather than against it. Raising the head of the bed by several inches, using a wedge or blocks under the bedposts rather than just extra pillows, keeps acid down during sleep. Quitting smoking strengthens the valve and benefits health broadly.
Identifying and moderating personal trigger foods, wearing looser clothing around the waist, and managing stress, which can heighten the perception of symptoms, round out the natural toolkit. For mild, occasional reflux, these measures often do the bulk of the work. It is fair to say that lifestyle change is not a minor add-on in GERD but a genuine treatment in its own right, and the foundation on which any medication is added.
Where to find natural support
The most reliable natural support for reflux comes from everyday habits and foods rather than special products. A reflux-friendly way of eating, smaller and earlier meals built around vegetables, whole grains, and lean protein, is widely accessible and costs nothing extra. The bedtime adjustments, such as raising the head of the bed, use simple household items.
Some traditional remedies, such as ginger tea, are gentle and harmless for most people and may bring comfort. Chewing sugar-free gum after meals can increase saliva and help clear acid, and is a simple, evidence-supported trick. Caution is wise, however, with strong herbal “reflux cures” marketed online, some of which have little evidence or can interact with medicines; a quick word with a pharmacist is sensible before trying them.
In short, the kitchen, the bedroom, and a few sensible daily habits are where the genuine natural support lives. Adjusting how and when you eat, keeping a healthy weight, not smoking, and using gravity to your advantage at night deliver the bulk of the benefit, while any remedy or supplement is, at most, a minor and carefully chosen extra.
When medical treatment is needed
When lifestyle measures alone do not control symptoms, or when the esophagus needs to heal, medicines are added, and several effective options exist. The mildest are antacids, which work by neutralising acid that is already in the stomach, giving quick but short-lived relief from occasional heartburn. They are useful for the odd flare rather than for daily, long-term control.

To actually reduce how much acid the stomach makes, two main drug groups are used. H2 blockers work by blocking histamine signals that stimulate acid-producing cells, lowering acid output and helping the esophagus heal to some degree. Proton pump inhibitors, or PPIs, such as omeprazole and similar medicines, act more powerfully by switching off the stomach’s acid pumps directly; they are the most effective at healing the esophageal lining and are often used for longer-term treatment. Both are available in some form over the counter and by prescription, and are generally safe, though, like all medicines, they have potential side effects worth discussing with a doctor, especially with long-term use.
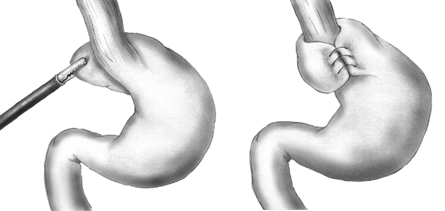
For the minority whose GERD does not respond to medicines, or who prefer not to take them long term, surgery is an option. The most common procedure, fundoplication, involves wrapping the top of the stomach around the lower esophagus to reinforce the valve and prevent reflux, and is usually done with minimally invasive keyhole techniques. In people with both obesity and GERD, weight-loss surgery can improve reflux as well. The common thread is that all of these treatments target either the acid or the faulty valve, are matched to the individual, and work best alongside, not instead of, the lifestyle foundations. Decisions about which to use belong with a doctor.
Small but effective daily changes
Keeping reflux under control usually comes down to a handful of steady habits rather than dramatic measures. Eating smaller portions, slowing down at meals, and finishing the last meal of the day at least two to three hours before bed remove some of the most common triggers. Keeping a simple note of which foods and situations spark symptoms helps each person fine-tune their own approach.
At night, raising the head of the bed and sleeping on the left side can reduce reflux during sleep, when symptoms often bite hardest. During the day, wearing looser clothing around the waist, staying upright after meals, and taking a short walk rather than slumping on the sofa all help keep acid where it belongs.
Over the longer term, working toward a healthy weight and not smoking are the two changes with the biggest payoff, addressing the root pressure on the valve. For those on medication, taking it as advised and reviewing with a doctor whether it is still needed prevents both under-treatment and unnecessary long-term use. Small, consistent steps like these turn reflux from a daily torment into a quietly managed background issue.
A final word
Acid reflux is so common that it is easy to dismiss, yet when it becomes frequent it deserves to be taken seriously, both for comfort and to protect the esophagus over the long run. The reassuring truth is that GERD is highly manageable: for most people, a combination of sensible eating habits, a few lifestyle adjustments, and, when needed, well-chosen medicines brings reliable relief. Seen this way, persistent heartburn is less a life sentence than a clear signal to adjust how and when you eat and to give that small, overworked valve a little help. This article is for general information only; for personal diagnosis and treatment, be sure to consult your physician.














