For most of the twentieth century, stomach ulcers were blamed on stress and spicy food, and patients were told to drink milk and relax. Then came one of medicine’s great surprises: the discovery that a bacterium, Helicobacter pylori, was behind most ulcers. That single insight transformed peptic ulcer disease from a chronic, recurring misery into a condition that can often be cured for good. A peptic ulcer is an open sore in the lining of the stomach or the first part of the small intestine, formed where the protective barrier has broken down and acid has eaten into the tissue beneath. In this article I explain what peptic ulcers are, which organs they affect, how they develop, their relationship with diet, and how they are healed by natural and medical means.
Table of Contents
- What is a peptic ulcer?
- What are the symptoms?
- Which organs does it affect?
- Progression: how an ulcer forms and advances
- How it presents and is diagnosed
- Causes and risk factors
- Its relationship with nutrition
- The place of fats
- Natural foods that support healing
- Supporting healing by natural means
- Where to find natural support
- When medical treatment is needed
- Small but effective daily changes
- A final word
What is a peptic ulcer?
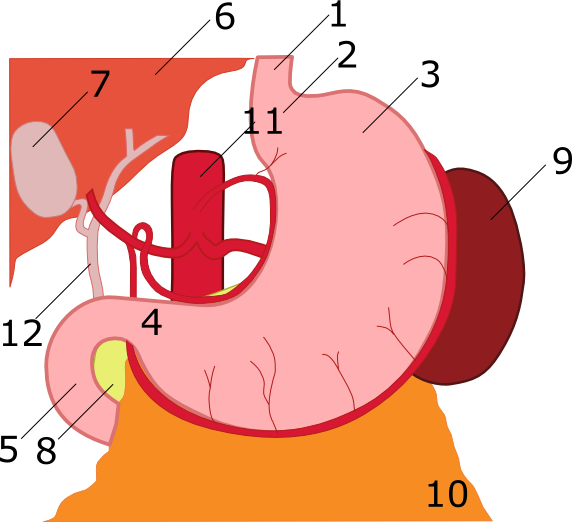
A peptic ulcer is a sore, or break, in the lining of the digestive tract where it is exposed to stomach acid. When it forms in the stomach itself, it is called a gastric ulcer; when it forms in the duodenum, the first stretch of the small intestine just beyond the stomach, it is called a duodenal ulcer. Both are grouped together under the term peptic ulcer disease.
To understand why ulcers form, it helps to appreciate the delicate balance inside the stomach. The stomach produces powerful acid and digestive enzymes to break down food, and at the same time it protects itself with a layer of mucus and other defences that keep that acid from digesting its own lining. An ulcer develops when this balance tips, either because the protective barrier is weakened or because something keeps irritating the lining, allowing acid to burn through to the tissue underneath.
The crucial modern understanding is that ulcers are not usually caused by acid alone, or by stress and diet as once thought. In the great majority of cases, the barrier has been undermined by one of two culprits: infection with H. pylori bacteria or the regular use of certain painkillers. Recognising ulcers as a problem of a damaged barrier, rather than simply excess acid, is what makes them so treatable today.
What are the symptoms?
The most common symptom of a peptic ulcer is pain or discomfort in the upper abdomen, somewhere between the breastbone and the navel. The pain is often described as dull, gnawing, or burning, and it characteristically comes and goes over days or weeks. For some people it appears when the stomach is empty or during the night and eases for a while after eating; for others, eating actually makes it worse.
Other symptoms reflect a stomach that is not working comfortably, including feeling full too quickly during a meal, uncomfortable fullness afterward, nausea, bloating, and belching. These indigestion-like symptoms can be mild and easy to brush aside, which is part of what makes ulcers easy to overlook in their early stages.
Importantly, many people with ulcers have no symptoms at all until a complication develops, and some warning signs demand urgent medical care. Black, tarry stools or blood in the stool, vomiting blood or material that looks like coffee grounds, sudden severe abdominal pain, dizziness or fainting, and a racing pulse can all signal bleeding or a perforation. These are emergencies, and anyone experiencing them should seek immediate help rather than wait.
Which organs does it affect?
The stomach and the duodenum are the primary organs involved, since these are the parts of the digestive tract most exposed to acid. An ulcer in either location can cause local pain and, if it bleeds, can lead to anaemia from slow blood loss or to a dramatic bleed if a larger vessel is eroded.
When an ulcer is left unchecked, its effects can spread beyond the lining. A deep ulcer can erode all the way through the wall of the stomach or duodenum, a perforation, which allows digestive contents to leak into the abdominal cavity and causes a severe, life-threatening infection. An ulcer near the outlet of the stomach can also cause swelling and scarring that block the passage of food, leading to vomiting and weight loss.

There is also a longer-term consideration. Chronic H. pylori infection, the main cause of ulcers, is itself linked with a small increased risk of stomach cancer over many years. This is one reason that diagnosing and eradicating the infection matters beyond simply healing the immediate sore. While most ulcers are entirely curable and most people do very well, these potential complications are exactly why persistent stomach symptoms deserve proper evaluation.
Progression: how an ulcer forms and advances
An ulcer begins quietly, usually with irritation and inflammation of the lining, sometimes called gastritis, before a true break in the surface forms. As the protective barrier weakens, acid reaches the deeper layers and an open sore develops. At this stage symptoms, if present, are typically the gnawing upper-abdominal pain and indigestion described earlier.
If the underlying cause persists, whether ongoing H. pylori infection or continued painkiller use, the ulcer can deepen and enlarge rather than heal. This is where complications begin to appear. A growing ulcer may erode a blood vessel and bleed, slowly or suddenly, or it may continue eating through the wall toward perforation.

The encouraging counterpoint is that this progression is highly preventable and, once the cause is removed, reversible. When H. pylori is eradicated or the offending painkiller is stopped, the lining can repair itself and most ulcers heal completely within weeks. Catching an ulcer before complications set in, and treating its root cause, is what turns a potentially dangerous process into a fully recoverable one.
How it presents and is diagnosed
Most often, a peptic ulcer presents as recurring upper-abdominal pain and indigestion that prompts a visit to the doctor. Because these symptoms overlap with reflux and ordinary dyspepsia, the doctor’s first task is to sort out the likely cause and to check for any warning signs that call for more urgent investigation.
The key diagnostic step is often testing for H. pylori, which can be done through a breath test, a stool test, or a blood test, and through samples taken during endoscopy. When symptoms are severe, persistent, or accompanied by alarm features such as bleeding, difficulty swallowing, or weight loss, doctors recommend an upper endoscopy. This involves passing a thin, flexible camera down into the stomach and duodenum to see the ulcer directly, take biopsies, and rule out other conditions.

This approach is both practical and reassuring. Younger people with typical symptoms and no warning signs can often be tested for H. pylori and treated without immediately needing endoscopy, while those with concerning features get a closer look. The same tests later confirm that the infection has been cleared and the ulcer has healed, closing the loop on treatment.
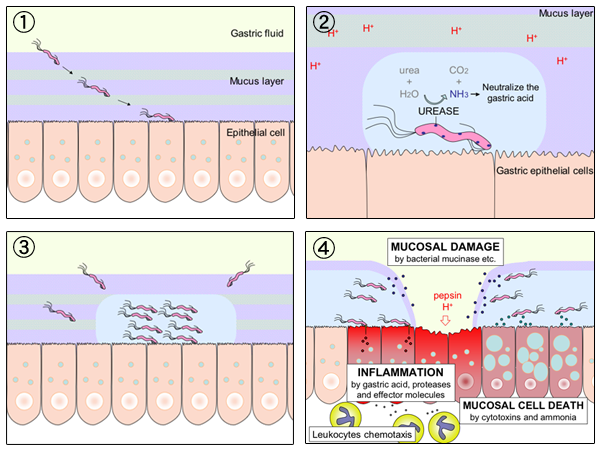
Causes and risk factors
Two causes account for the overwhelming majority of peptic ulcers. The first is infection with Helicobacter pylori, a spiral-shaped bacterium that lives in the stomach lining, weakens its protective barrier, and provokes inflammation. Many people carry H. pylori without ever developing an ulcer, but in those who do, eradicating the bacteria usually cures the disease.
The second major cause is the regular use of nonsteroidal anti-inflammatory drugs, or NSAIDs, a group that includes common painkillers such as aspirin, ibuprofen, and naproxen. These medicines relieve pain and inflammation, but they also undermine the stomach’s protective lining, making it more vulnerable to acid. The risk rises with higher amounts, longer use, taking more than one such drug, and combining them with H. pylori infection.
Less common causes include certain other infections, some medicines such as corticosteroids and particular antidepressants especially when combined with NSAIDs, and rare conditions that drive the stomach to produce excessive acid. Smoking slows ulcer healing and raises the risk, and heavy alcohol use can irritate the lining. Knowing these causes is empowering, because the two biggest ones are both addressable: an infection that can be treated and a class of medicines that can often be adjusted.
Its relationship with nutrition
The understanding of diet and ulcers has changed dramatically. For decades, spicy food, coffee, and stress were blamed, and bland diets were prescribed. We now know that food does not cause ulcers, and that the old bland diets do little to heal them. Diet’s real role is more modest but still meaningful: certain foods and habits can aggravate symptoms or support comfort and healing, even though they are not the underlying cause.
Some people find that spicy foods, very acidic foods, caffeine, and alcohol worsen their pain, while others tolerate them without trouble. Rather than following a rigid list, it makes sense to notice one’s own triggers and to moderate those specifically. Alcohol and smoking, however, genuinely interfere with healing and are worth avoiding while an ulcer recovers.
There is also growing interest in foods that may support the stomach lining and even discourage H. pylori. Moving away from heavy alcohol and excessive irritants, while eating a balanced diet built around vegetables, fruits, whole grains, and lean protein, gives the lining the best environment to repair. In short, diet is a supportive player in ulcer care, not the villain it was once made out to be, and not a substitute for treating the real cause.
The place of fats
Fat deserves a balanced word in the context of ulcers, free of the old myths. There is no good evidence that dietary fat causes ulcers or that cutting it out heals them. What matters more is the kind of fat and the company it keeps, since very greasy, heavy meals can sit uncomfortably and aggravate symptoms in a stomach that is already sore.
It is worth remembering that fat is an essential nutrient the body genuinely needs. It builds the membrane of every cell, is a raw material for hormones, and is required to absorb the fat-soluble vitamins A, D, E, and K. The goal is never to eliminate fat but to choose good sources and reasonable portions. Healthy fats from olive oil, nuts, avocado, and fish are part of a nourishing diet and are very different from the spoiled and repeatedly heated fats found in fried and ultra-processed foods, which add irritation and inflammation without benefit.
The familiar “fat-free” trap applies here too: many low-fat products replace the missing fat with extra sugar or refined starch, offering empty calories rather than genuine nourishment. For someone recovering from an ulcer, the sensible path is to favour quality fats in modest amounts, avoid very greasy meals that provoke discomfort, and steer clear of heavily processed substitutes, rather than fearing fat in all its forms.
Natural foods that support healing
While no food can cure an ulcer on its own, several foods may support a healthy stomach lining and a comfortable recovery. Foods rich in fibre, such as vegetables, fruits, whole grains, and legumes, are associated with better digestive health and may help protect against ulcers. Brightly coloured fruits and vegetables supply antioxidants that support tissue repair.
Certain foods have attracted particular interest for the stomach. Foods containing beneficial compounds, such as cruciferous vegetables and some fermented foods rich in probiotics like yoghurt, have been studied for their potential to support the lining and, in the case of probiotics, to help the body cope with H. pylori alongside medical treatment. Honey and certain herbs have traditional reputations as soothing, though they are supportive rather than curative.
The common thread among ulcer-friendly foods is that they are whole, gentle, and nourishing, supporting repair without irritating a tender stomach. Equally important is the pattern of eating: smaller, regular meals are often more comfortable than large ones, and avoiding alcohol and excessive caffeine while the ulcer heals gives the lining a calmer environment. Building everyday meals around this kind of pattern works hand in hand with treating the underlying cause.
Supporting healing by natural means
It is important to be honest here, because peptic ulcers are a condition where natural measures support recovery but usually cannot replace medical treatment. When an ulcer is driven by H. pylori, the infection needs to be cleared with medicines; when it is driven by NSAIDs, those medicines need to be addressed. No diet or remedy alone will reliably heal an ulcer if the underlying cause continues unchecked.
Within that honest framing, natural habits genuinely help. Stopping smoking is one of the most valuable steps, since smoking slows healing and raises the risk of recurrence. Moderating or avoiding alcohol gives the lining a chance to repair. Managing stress does not cure ulcers, but since stress can heighten the perception of symptoms and affect habits, it is worth attending to for overall comfort.
Eating smaller, regular meals, identifying and avoiding personal trigger foods, and including supportive foods such as fibre-rich plants and probiotic-containing yoghurt can all make recovery smoother. The honest message is that lifestyle is a real and helpful ally that supports healing and prevents recurrence, while the medicine that treats the cause is what actually allows the ulcer to close. The two are partners, not rivals.
Where to find natural support
The most reliable natural support for ulcer recovery comes from everyday foods and habits rather than special products. A balanced diet rich in vegetables, fruits, whole grains, and lean protein is widely available and gives the lining what it needs to repair. Plain yoghurt and other probiotic-containing foods are easy additions that may support the gut, especially alongside antibiotic treatment for H. pylori.
Some traditional remedies, such as certain herbal teas or honey, are gentle and harmless for most people and may bring comfort, though they are supportive rather than curative. Caution is wise with strong herbal “ulcer cures” sold online, some of which have little evidence or can interact with medicines; a quick conversation with a pharmacist is sensible before trying them.
In short, the kitchen and a few sensible habits are where the genuine natural support lives. A nourishing diet, avoiding smoking and excess alcohol, and eating in a calm, regular pattern deliver real benefit and help prevent recurrence, while any supplement or remedy is, at most, a minor and carefully chosen extra alongside proper treatment of the cause.
When medical treatment is needed
For nearly everyone with a peptic ulcer, medical treatment is central, because it both heals the sore and removes its cause. The first goal is to reduce stomach acid so the lining can repair. Proton pump inhibitors, or PPIs, such as omeprazole and similar medicines, do this powerfully by switching off the stomach’s acid pumps, and they are the mainstay of ulcer healing. H2 blockers, which lower acid by blocking histamine signals to the acid-producing cells, are a gentler alternative used in some situations.

The second, equally important goal is to treat the underlying cause. When H. pylori is present, doctors prescribe a combination treatment, typically two or more antibiotics together with a PPI, and sometimes a bismuth compound, taken as a course over a couple of weeks. Taking every dose exactly as prescribed is vital, because stopping early can let the bacteria survive and develop resistance. After treatment, a follow-up test confirms the infection has truly been cleared.
When NSAIDs are the cause, the approach is to stop them if possible, switch to a gentler pain option, or, if they must be continued, add a protective PPI. In the rare cases where ulcers do not heal, keep returning, or cause complications such as bleeding or perforation, endoscopic procedures or surgery may be needed, usually in hospital. The common thread is that modern treatment targets both the acid and the root cause, is matched to the individual, and is highly effective. Decisions about which medicines to use belong with a doctor.
Small but effective daily changes
Recovering well from an ulcer and preventing its return comes down to a few steady habits. For those prescribed treatment, the single most important one is completing the full course of medicine exactly as directed, especially the antibiotics used to clear H. pylori, even once the pain has gone. Stopping early is the most common reason treatment fails.
Beyond medication, being thoughtful about painkillers makes a real difference. Anyone prone to ulcers should use NSAID painkillers sparingly, discuss safer alternatives with a doctor or pharmacist, and never assume that over-the-counter status means they are harmless to the stomach. Quitting smoking and moderating alcohol both speed healing and lower the chance of recurrence.
Day to day, eating smaller, regular meals, noticing and avoiding personal trigger foods, and including supportive foods such as fibre-rich plants and probiotic yoghurt all help keep the stomach comfortable. Keeping a simple note of symptoms and reporting any warning signs promptly ensures that problems are caught early. Small, consistent steps like these, combined with proper treatment of the cause, turn peptic ulcer disease from a recurring ordeal into a one-time, fully resolved episode for most people.
A final word
The story of peptic ulcers is, in many ways, a hopeful one. A condition once thought to be a lifelong burden of stress and diet turned out, for most people, to be a curable infection or a reaction to a particular kind of painkiller. With the right treatment, the underlying cause can be removed and the lining can heal completely, often for good. Seen this way, persistent stomach pain is not something to silently endure but a clear signal to get checked, because the answer is usually both findable and fixable. This article is for general information only; for personal diagnosis and treatment, be sure to consult your physician.














